- Narendra Kotwalnarendrakotwal at gmail dot comDepartment of Endocrinology, Army Hospital (R&R), Delhi Cantt, New Delhi, India
- Yogesh Kumaryogeshrewari77 at gmail dot comDepartment of Endocrinology, Army Hospital (R&R), Delhi Cantt, New Delhi, India
- Aditi Panditp_aditi at hotmail dot comDepartment of Endocrinology, Army Hospital (R&R), Delhi Cantt, New Delhi, India
- Vimal Upreti #v_upreti123 at rediffmail dot comDepartment of Endocrinology, Army Hospital (R&R), Delhi Cantt, New Delhi, India
Pituitary apoplexy is identified as one of the factor responsible for self regression of pituitary adenomas though it is seen rarely in acromegaly. Head injury is one of the rare precipitating factors for pituitary apoplexy. Here we report a case of acromegaly who developed pituitary apoplexy following mild head injury with and subsequently had remission of acromegaly with and development of panhypopitutarism.
Apoplexy in pituitary tumor is an uncommon complication due to either bleed or infarction within a pre-existing pituitary adenoma. The incidence of pituitary apoplexy is reported in 0.6-10.5% of all the cases of pituitary adenomas [1]. Most cases of pituitary apoplexy are seen in nonfunctioning pituitary adenomas. Among functioning pituitary adenomas, prolactinomas are the commonest to show apoplexy. Apoplexy in somatotropinomas is rarely reported in literature with estimated incidence of 3.5-4% [2]. Head injury is considered as one of the rare causes of pituitary apoplexy [3]. Herein, we describe a rare case of acromegaly who developed pituitary apoplexy in pituitary macroadenoma following mild head injury with subsequent development of panhypopituitarism and remission of acromegaly and diabetes mellitus.

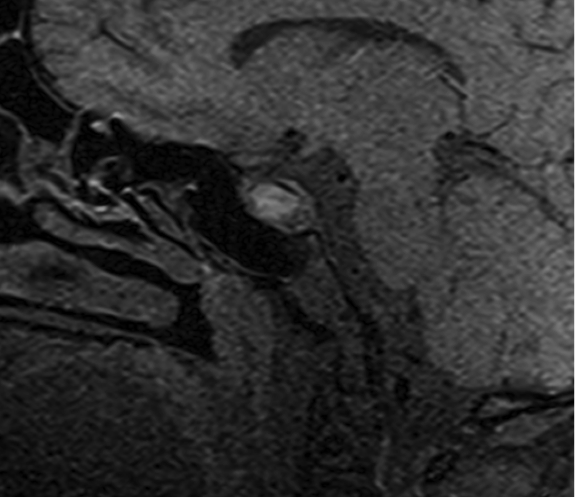
A 42-year-old male, diagnosed case of diabetes mellitus for 03 years on oral antidiabetic drugs (OADs) was referred to our centre for inadequate glycemic control (blood glucose - F/PP: 182/278 mg/dl and HbA1c 9.1%). At our Endocrinology clinic, he was noted to have acromegaloid features (acral enlargement, coarse facial features, large fleshy nose, prognathism, deep naso- labial folds, occipital protuberance, macroglossia, fleshy lips and nose, increased interdental distance) (Figure 1), was provisionally diagnosed as having acromegalyand was advised work up accordingly. Investigations revealed non-suppressible growth hormone to 75 gm glucose load (GH basal 26.1 ng/ml, one hour post load 24.6ng/ml; normal response<1 ng/ml); hence, he was advised other pituitary hormones (that were normal) and magnetic resonance imaging (MRI) of sella. While under investigations, he met with a road traffic accident and presented with transient loss of consciousness and multiple abrasions. Clinically, he had Glasgow Coma Scale of 14 (Score: 3 – coma, 15 – normal) with no focal neurological deficit and was classified as mild head injury, rest of the general and systemic examination was non contributory. MRI of brain revealed pituitary macroadenoma sized 13x21x10.5mm with intratumoral bleed (Figure 2).
Six weeks after recovering from head injury, hormonal analysis was repeated that revealed suppressible GH response post glucose load (GH levels at 60 minutes – 0.44 ng/ml; normal <1ng/ml); secondary adrenal insufficiency [ basal cortisol 0.39ug/dl (Normal 12 -25ug/dl), one hour post ACTH cortisol levels 3.71 ug/dl (Normal >18ug/dl)]; secondary hypogonadism [ (LH 0.01IU/L(Normal 2.5-9.8IU/L), FSH 0.79 IU/L (Normal 1.0-12IU/L), Testosterone 0.06ng/dl (Normal 3.0-12ng/ml)]; secondary hypothyroidism [ T4 4.1ug/dl (Normal 5.5-13.5ug/dl), TSH 0.1 uIU/ml (Normal 0.5 – 6.5uIU/ml)] and low prolactin levels [ (2 ng/ml) (Normal <25ng/ml)]. Hydrocortisone, Levothyroxin and testosterone supplementation was started and patient was kept under follow up. Revaluation after 03 and 06 months showed suppressible GH on glucose loads and more than 50% regression in size of pituitary lesion on MRI of sella (Figure 3). There was resolution of clinical features and patient became euglycemic without medications and he is clinically euhormonal on hormonal replacement.

Pituitary apoplexy is a rare medical emergency caused commonly due to blood pressure alteration, pituitary irradiation, dopamine agonist treatment, pituitary stimulation test and pregnancy. Among several precipitating factors identified, head injury is one of the rare precipitating factor for pituitary apoplexy [3]. Pituitary apoplexy is identified as one of the known causes of spontaneous regression of pituitary tumor [4]. The increased pressure inside the tumor cavity due to hemorrhage may compromise the vascular supply [5] and cause the infarction secondarily, leading to regression by tumor necrosis [4]. Pituitary apoplexy may compromise pituitary hormonal functions partially or completely. The mechanism of pituitary apoplexy following head injury is not well recognized. One of the possible mechanism may be direct shearing force between tightly fixed intrasellar and relatively free suprasellar part of the tumor due to head trauma [3]. The other mechanism could be direct injury by adjacent bony structures [3]. In our case the shearing force due to head trauma has most likely caused the pituitary apoplexy as there was no obvious skull fracture or bony injury and has led to remission of acromegaly and subsequent normalization of secondary diabetes mellitus and has resulted in panhypopituitarism requiring hormonal replacement.
- Bills D, Meyer F, Laws E, Davis D, Ebersold M, Scheithauer B, et al. A retrospective analysis of pituitary apoplexy. Neurosurgery. 1993;33:602-8; discussion 608-9 pubmed
- Thomas N, Simon R, Chacko G, Chacko A, Chandy M, Seshadri M. Regression of acromegaly following pituitary apoplexy. Neurol India. 1999;47:161-2 pubmed
- Horie N, Tokunaga Y, Takahashi N, Furuichi S, Mori K, Shibata S. [A case of pituitary apoplexy with severe consciousness disturbance following mild head trauma]. No To Shinkei. 2002;54:697-701 pubmed
- Bjerre P, Lindholm J, Videbaek H. The spontaneous course of pituitary adenomas and occurrence of an empty sella in untreated acromegaly. J Clin Endocrinol Metab. 1986;63:287-91 pubmed
- Nishioka H, Haraoka J, Miki T. Spontaneous remission of functioning pituitary adenomas without hypopituitarism following infarctive apoplexy: two case reports. Endocr J. 2005;52:117-23 pubmed